INTRODUCTION
While common peroneal nerve entrapment is a well-recognized pathology, symptomatic entrapment of the superficial peroneal nerve (SPN) is rare and a more elusive clinical entity with a less established treatment plan4). SPN entrapment was first described by Henry6) who observed that the pain could be reproduced by compressing the nerve at the point where it emerged from the deep fascia. In 1960, Kopell and Thompson7) suggested the site of entrapment where the SPN pieces the deep fascia in the distal leg. Styf and Morberg12) demonstrated the rarity of this entrapment syndrome in 1997. The incidence of SPN entrapment was 3.5% of 480 patients with chronic leg pain. In addition, they reported an 80% success rate with decompression of the SPN12). Successful results of SPN decompression have been repeatedly reported since the report of Styf and Morberg.
The diagnosis and treatment of SPN compression have not been as clearly defined. Sensory disturbance of the dorsum of the foot or lateral lower leg without corresponding weakness of the peroneus muscles is hallmark of the entrapment of the superior peroneal nerve1). Diagnosis is made mostly based on the clinical symptoms because it is difficult to diagnose with nerve conduction studies4,8,12). Because there are multiple potential sites of peroneal nerve entrapment, it is difficult to ascertain whether potential compression sites are involved or whether the nerve is simply aggravated by the more proximal compression1). Entrapment of the superficial and common peroneal nerves may be concurrent. Franco et al.4) reported that 78% of patients with decompression of the SPN had been treated previously by common peroneal nerve decompression surgery. We report a patient who presented with chronic neuropathic pain in the left lower leg and foot, was diagnosed with isolated SPN entrapment, and was successfully treated with decompression surgery.
CASE REPORT
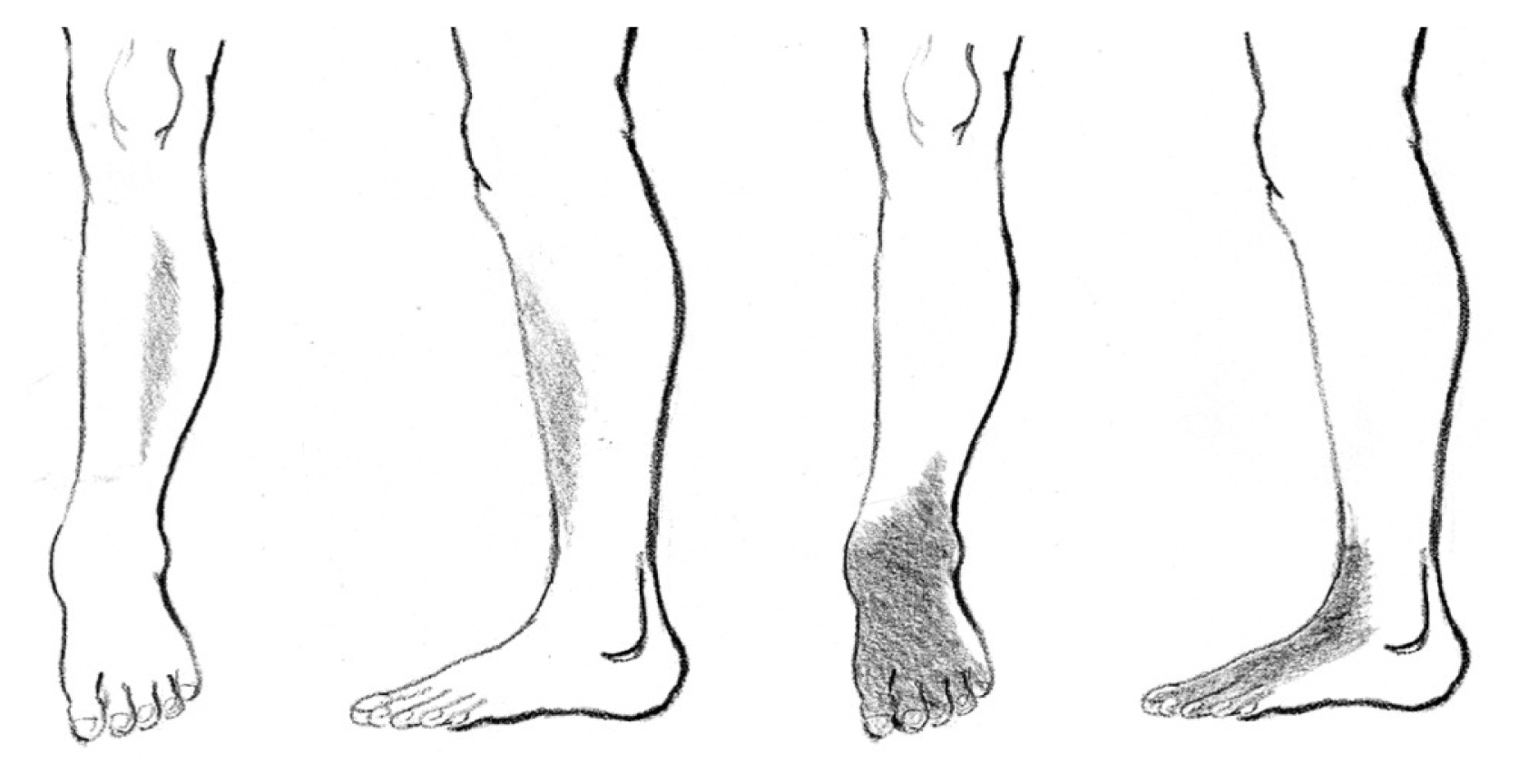
A 73-year-old male patient presented with burning and tingling pain in the left ankle and dorsum of the foot lasting 2 years. Two years ago, while he was squatting to work, a dull, slightly numb sensation suddenly developed in his left lower leg lateral to his shin (Fig. 1). This dull pain continued and was uncomfortable, but it did not interfere with the movement of the left leg and was not very severe. It lasted for 2 months and went away spontaneously without any special treatment. Six months later, while he squatted back to work, a stiff pain suddenly occurred in the previous painful area of his left lower leg. At the same time, burning pain and tingling sensation occurred in his ankle, dorsum of the foot, and toes (Fig. 1). The pain in his left lower leg and foot, which occurred again, did not improve naturally and lasted all day. The pain did not cause gait disturbance but got slightly worse as he walked. Over time, the stiffness in the left lower leg disappeared gradually, but the burning pain in his left ankle and the dorsum of left foot persisted.
Two years after the occurrence of pain, the pain in the left ankle and foot became more severe, which interfered with activities of daily life and work. He was diagnosed with lumbar spinal stenosis at several orthopedic clinics and was treated with regular medications and epidural blocks without any improvement. Finally, electromyography (EMG) was recommended at a hospital for suspicion of peripheral nerve abnormalities. He was referred to the present author as abnormality in the conduction velocity of the SPN was confirmed by the examination.
On examination, there was no weakness of eversion of the left foot. Neither restriction of lumbosacral range of motion nor complaints of low back pain and ankle was observed. No tenderness or Tinel sign was evoked along the course of the peroneal nerve in the left lower leg. However, allodynia to light touch was elicited in his left ankle and dorsum of the foot. Mild hypesthesia was observed in the painful area. His pain was always present regardless of leg movement and posture and did not improve with rest. There was no pain induced by passive movement of the knee or ankle. However, he reported that the pain worsened after walking and momentarily became very severe when squatting. Sciatic root stretch signs were negative and the deep tendon reflex was normoactive.
An EMG and nerve conduction study of the lower extremity performed at one hospital showed an absence of discernible waves in the left SPN. However, no abnormality was found in the amplitudes of the tibialis anterior and peroneus muscles. Magnetic resonance imaging (MRI) of the left knee and ankle did not reveal any lesions that could explain the patient’s pain. X-ray findings of the left knee, ankle, and foot were nonspecific. Laboratory examinations including erythrocyte sedimentation rate, C-reactive protein, rheumatoid factor, antinuclear antibody, and creatinine kinase were normal. Considering the course of neuralgia of the left SPN and abnormal EMG findings, an exploration of the left SPN was performed.
A 20cm-long, longitudinal skin incision was made two fingerbread ths lateral to the apex of the tibia, centering on the area where the initial pain occurred, 10 cm proximal to the lateral malleolus, as previously suggested (Fig. 2A)1,4). The anterior intermuscular septum was easily identified after dissection of the subcutaneous layer (Fig. 2B). The SPN was identified under the fascial envelope lateral to the anterior intermuscular septum(Fig. 2B). The superficial fascia was divided longitudinally, revealing a V-shaped interfascial space within which the nerve run. In the distal side of the incision, the location of nerve entrapment was identified just prior to the bifurcating point into the intermediate and medial dorsal cutaneous sensory nerves (Fig. 2C). Proximal dissection along the course of SPN did not reveal any suspicious area of entrapment. After securing complete dissection of the proximal and distal course of the nerve, the fascial septum underlying the nerve was divided with four cuts to completely loosen the fascial tunnel (Fig. 2D). There were no anatomical variations, such as the passage of the SPN within the anterior compartment3).
The allodynia in the left leg temporarily worsened for 2 weeks after the operation and then gradually improved until a month. The patient’s condition was stable without any recurrent symptoms at the 12-month follow-up at an outpatient clinic.
DISCUSSION
1. Anatomy of the SPN and Its Entrapment
The SPN(superficial fibular nerve) begins at the bifurcation of the common peroneal nerve. It lies deep to the peroneus longus at first, then passed anterio-inferiorly between the peroneus longus and brevis muscles and extensor digitorum longus, and pierces the deep fascia in the distal third of the leg11). It divides onto a large medial dorsal cutaneous nerve and a smaller, laterally placed, intermediate dorsal cutaneous nerve, usually after piercing the deep fascia, but sometimes while it is still deep to the fascia11). As the nerve lies between the muscles, it supplies the peroneus longus and brevis muscles and the skin of the lower leg.
The medial dorsal cutaneous nerve passes in front of the ankle joint and divides into two dorsal digital branches; one supplies the medial side of the hallux and the other supplies the adjacent side of the second and third toes10,11). It communicates with the saphenous and deep peroneal nerves. The smaller intermediate branch crosses the dorsum of the foot laterally. It divides into dorsal digital branches that supply the contiguous sides of the third to fifth toes and the skin of the lateral aspect of the ankle, where it connects with the sural nerve. Therefore, branches of the SPN supply the skin of the dorsum of all the toes except that of the lateral sided of the fifth toe (supplied by the sural nerve) and the adjoining sides of the great and second toes (supplied by the deep peroneal nerves).
A lesion of the SPN causes weakness of foot eversion and sensory loss on the lateral aspect of the leg that extends on to the dorsum of the foot. The nerve can be subjected to entrapment as it penetrates the deep fascia of the leg and it may also be involved in compartment syndrome that affects the lateral compartment of the leg10). The path of the SPN varies significantly, traveling through the lateral compartment only, the anterior compartment, or both compartments3,10,11). A cadaveric anatomical study revealed that the SPN branched before piercing the crural fascia in 35% of the specimens, and in all these specimens the medial dorsal cutaneous nerve of the foot was located in the anterior compartment while the intermediate dorsal cutaneous nerve of the foot was located in the lateral compartment10). In addition, in 35% of specimens, the intermediate dorsal cutaneous nerve of the foot was absent or did not innervate any toe. The sural nerve supplied the superficial innervation to the lateral half of the foot and toes in 40% of the specimens10).
As it exits though the deep fascia at the distal third of the leg, where it divides into the medial and intermediate dorsal cutaneous nerve branches, the fascia area where the nerve pass though creates a site for entrapment3,5,10,11). This site of stenosis is further exacerbated by muscle hypertrophy, displaced fractures, direct trauma, mass effect, edema, and inversion injuries10).
2. Diagnosis
Sensory disturbance of the dorsum of the foot or lateral lower leg without corresponding weakness of the peroneus muscles is hallmark of the entrapment of the superior peroneal nerve1). The pain is aggravated by forceful inversion of the foot, which causes traction of the nerve against its entrapment site as it pierces the deep fascia of the distal leg. In addition, exacerbation of the symptoms by walking and exercise is common. Positive Tinel sign and transient improvement of the pain by local blockade of the SPN are diagnostically useful1,8). The reported etiologies of SPN entrapment include muscle herniation, trauma, mass lesions such as lipoma and varicose vein, and idiopathic8).
Nerve conduction studies may be useful in demonstrating a local conduction defect along the course of the SPN in the absence of findings at the fibular head1,2,9). The normal function of the extensor digitorum brevis (EDB) is expected with preserved first web space sensation1,2,9). Except for the cases with mass lesions, the use of MRI, ultrasound, and other imaging modalities is not routinely performed4).
3. Considerations in Surgical Treatment
To prevent placing the SPN under tension, conservative treatment involves immobilization and limiting inversion and plantar flexion10). A corticosteroid injection can be diagnostic and therapeutic. If conservative treatment fails, then surgical treatment involves the release of the entrapment site of the SPN10).
The first thing to consider when performing decompression surgery is that the entrapment of the SPN may be multiple. As can be seen in the report of Franco et al.4), 78% of their patients who underwent SPN decompression surgery had combined simultaneous decompression of the common peroneal nerve. They hypothesized that an area proximal to the compression site might render areas further downstream more susceptible to compression (double crush phenomenon)4,8). Indeed, 5 patients reported in another case series also underwent common peroneal nerve decompression prior to SPN decompression8). According to Franco et al.4), those patients who had only decompression of the SPN without common peroneal release showed negative provocative maneuvers at the fibular head region, no motor weakness, and no electrophysiological evidence of motor disturbance. In the present case, no motor weakness was clinically confirmed, only sensory symptoms and pain of the SPN distribution, and no motor disturbance was identified in the EMG. In addition, as no mass lesion was found in the MRI, only decompression surgery of the SPN was performed.
The next consideration when performing decompression for the SPN entrapment is the possibility of anatomical variation of the nerve and complete decompression of its proximal and distal course1,3,10). An important anatomical variation to recognize is the accessory peroneal nerve from the SPN, which contributes innervation to the EDB in approximately one-third of the population2,9). Long incisions in the front of the lower leg (up to 18 cm), as suggested by experienced authors1), may be a little burdensome. However, a long incision along the course of the SPN seems inevitable to ensure complete decompression of the nerve penetration site of the deep fascia and to check the anatomical variations and possible communication branches leading to the anterior compartment1,3,10). For example, in Matsumoto et al.’s report8), a small incision in the first operation for SPN entrapment focused on the fascial entrapment site caused an insufficient nerve resulted in recurrence of the symptoms requiring additional decompression. A fasciotomy for the anterior and lateral compartment was recommended for complete loosening of the fascial entrapment site of the SPN and the fascial tunnel1,4). Some authors recommend decompression of all three sites of possible entrapment of the superficial peroneal and common peroneal nerve pathways for successful pain relief1).