INTRODUCTION
Common peroneal neuropathy (CPNe) is a usual cause of dropped foot, which results from various causes, including idiopathic causes, iatrogenic causes, tumors, and trauma. Taking detailed patient history and performing neurological examination are the most important initial clinical approaches to reach a diagnosis of suspected CPNe, while final diagnostic confirmation depends on the electrodiagnostic study (EDX)1,7,14).
As neuropraxic lesions rarely show positive electromyographic finding5), for EDX, patients have to wait for confirmation of diagnosis until Wallerian degeneration initiates after the onset of symptom; thus, it could take a certain amount of time to establish the diagnosis. In contrast, magnetic resonance imaging (MRI) requires no such delay to find denervation and has played an important role in the detection and characterization of pathological conditions of skeletal muscles that change muscle signal intensity4).
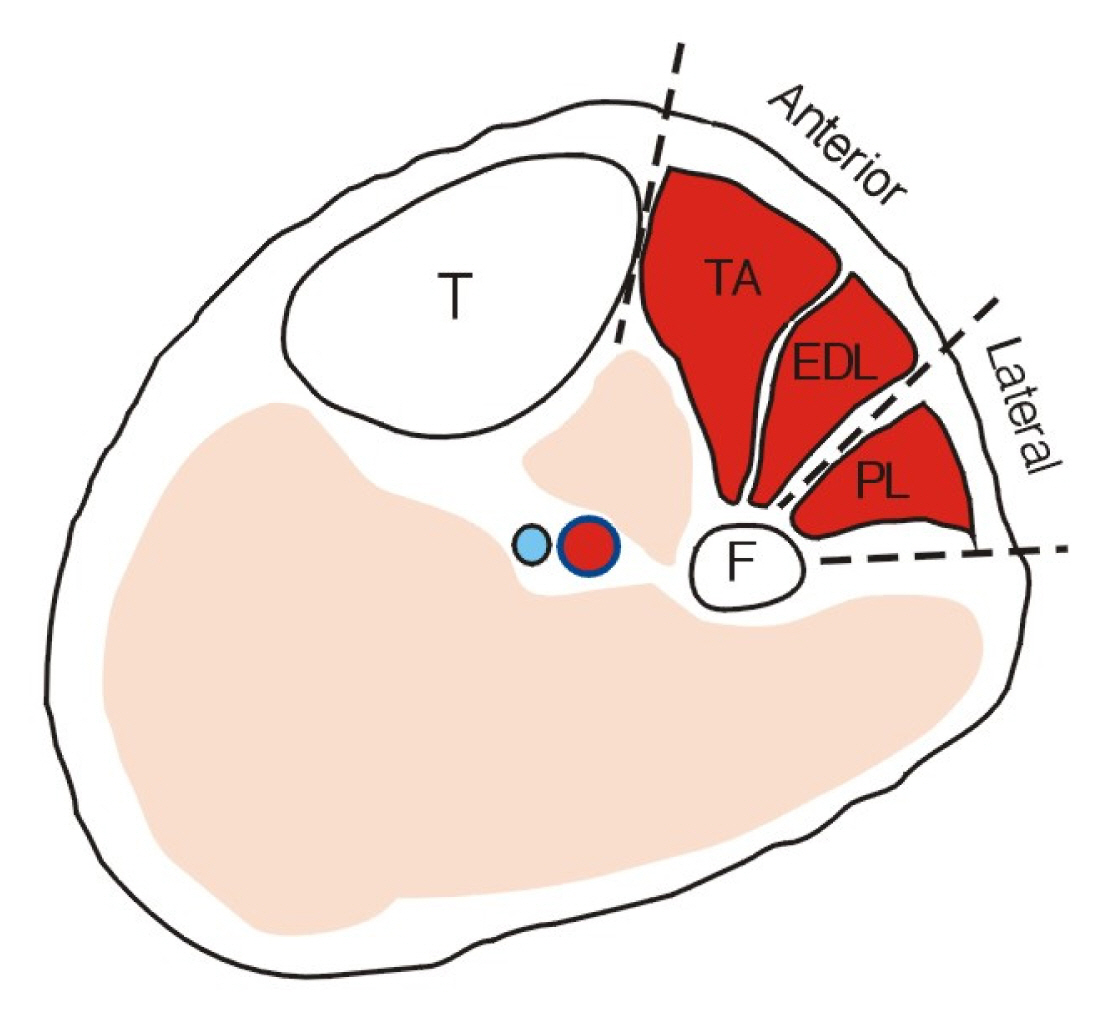
The CPNe innervates the muscles of the anterior and lateral compartments of the lower leg1). Peroneus longus is situated in the lateral compartment and both extensor digitorum longus and tibialis anterior in the anterior compartment3) (Fig. 1). Using conventional MRI, CPNe can be diagnosed with signal changes from denervation of these muscles.
For 3 years, the current study’s authors performed conventional knee MRI in patients with CPNe and found signal changes in the muscles in the antero-lateral compartment during diagnostic process. The purpose of this study was to assess the clinical applicability of MRI for the early diagnosis of patients with CPNe.
MATERIALS AND METHODS
We retrospectively examined medical records of 58 patients diagnosed with CPNe confirmed by clinical approaches or EDX from December 2017 to December 2020. Among these patients, 35 underwent axial MRI with a 1.5-Tesla scanner (Gyroscan Intera; Philips Medical Systems, Best, the Netherlands) from the apex of the popliteal fossa to 20 cm distal from the fibular head. Only these subjects were included in the study.
Patients were classified into three chronological groups according to the time of examination after the occurrence of dropped foot—acute, subacute, and chronic onset groups. Patients in the acute onset group underwent examination within the first 1 to 2 weeks of onset, those in the subacute onset group underwent examination within 3 to 4 weeks of onset, and those in the chronic onset group underwent examination after >4 weeks of onset.
MRI was performed for all the subjects for this study immediately after the initial clinical evaluation. The muscle findings of MRI were chronologically classified as shown in Table 1. Short tau inversion recovery (STIR) images are highly water-sensitive, and the timing of the pulse sequence used suppresses signals coming from fatty tissues; therefore, only water molecules are visualized bright. The acutely and subacutely denervated muscle shows a high-signal intensity pattern on fluid-sensitive sequences and normal signal intensity on T1-weighted MRI because of muscle edema. In chronic denervation, muscle atrophy and fatty infiltration demonstrate high signal changes on T1-weighted sequences association with volume loss. Effectively applicable ranges of muscle volume to define atrophy, of muscle/fat infiltration ratio to define atrophy, and of the degree of signal intensity to define muscular edema were not available in other literatures. This problem could have been solved if we compared the MRI of the affected side to that of the unaffected side, but we could not perform the MRIs of both knees due to the longer time required and the financial reason. Therefore, we depended upon the radiologist’s reading and the double-checking from 2 of the authors (C.G.Y. and Y.J.S.).
All patients underwent EDX 4 weeks after onset. If the neuropathy was chronic, the patient underwent EDX immediately. The result of delayed nerve conduction velocity (NCV) was subdivided into muscle denervation and without. The study was approved by Chuncheon Sacred Heart Hospital Institutional Review Board.
RESULTS
1. Baseline Characteristics
Table 2 represents the demographic data of the patients. The sample showed 2:1 ratio between male and female. The patients’ age ranged from 25 to 76 years, and the mean age was 49.3 years. The etiologies of CPNe were idiopathic in 32 patients (91.4%) and traumatic in 3 patients (8.6%). In 3 patients with traumatic CPNe, there was no direct injury to the musculature related to the CPN. The modes of trauma were fibular fracture in 2 patients and laceration of the knee in 1 patient. We could not find a significant difference in the affected laterality. The chronicity of the CPNe was: acute in 18 (51.4%); subacute in 11(31.4%); chronic in 6 (17.1%) patients.
2. MRI Appearances of the Muscles
MRI showed positive findings in 32 cases. The classified findings are summarized in Table 3. The affected muscles were: multiple muscles in the anterolateral compartment simultaneously in 30 cases; single muscle (peroneus longus) in two cases. CPNe could be diagnosed using MRI in about 91%(32/35) of all the cases. Excluding the chronologically chronic stage, the diagnosis rate was approximately 90%(26/29) of all the cases. The MRI changes in the affected muscle included a high-signal intensity in fluid-sensitive sequences (T2-weighted and STIR images) in 23 cases and a high-signal intensity of fat infiltration and atrophy with decreased muscle volume (T1-and T2-weighted images) in 9 cases.
3. EDX Results
All the patients showed abnormality in the NCS, but in 8 patients, normal electromyography (EMG) was obtained. In the acute onset group, eight cases had delayed latency of NCV with normal EMG. In the remaining 27 cases (77%), positive sharp waves and acute fibrillation were noted, confirming muscle denervation.
DISCUSSION
The common peroneal nerve (CPN), a branch from the sciatic nerve, descends obliquely along the lateral side of the popliteal fossa to the head of the fibula and then winds around the neck of the fibula. The CPN enters the anterior and lateral muscle compartments of the leg and gives branches. These include superficial peroneal nerve, which innervates peroneus longus and brevis for ankle eversion; deep peroneal nerve, which innervates the tibialis anterior for ankle dorsiflexion as well as the extensor digitorum longus and brevis for toe extension1,7,13,14). We thought the connection between the CPN and the muscles might lead to the diagnostic potential of MRI by identifying alterations in muscles.
During muscle denervation, muscle blood content increases as the intramuscular capillary bed get proliferated. Also, extracellular fluid within the denervated muscle cells increases, probably due to increased cell membrane permeability and reduced Na-K-ATPase function2,8,10). Therefore, abnormalities are seen in the denervated muscles on water-sensitive MRI sequences4,6,9,12). Peripheral nerve injury also induces metabolic changes. Glucose metabolism takes place in the way that new glucose uptake is inhibited while glycolysis is activated. Furthermore, proteolysis increases10). These metabolic changes result in morphological change, shown as atrophy. This phenomenon occurs as soon as the nerve gets damaged and can also be demonstrated histologically as a reduction in the muscle fiber diameter. As atrophy progresses, the ratio of fat to protein tends to increase2,6,8,10). Therefore, we can see the shrinkage of muscle bulk and the fatty infiltration within the muscle in chronic denervation. In experimental studies, moderate atrophy was seen as early as approximately 10 to 12 days after denervation. However, it typically takes 3 weeks after the insult to the nerve to observe pathognomonic findings histologically8).
Several clinical and experimental studies have demonstrated signal changes in the denervated muscles on MRI3,4,6,12). An animal-based study demonstrated that changes could be observed on MRI as early as within as 24 hr after injury6). In a clinical study, an abnormality from denervation could be demonstrated within 4 days of injury12). In this study, we performed a conventional axial MRI of the knee, which revealed the degree of muscle denervation according to its time course. In three cases, however, we could not find any signal changes in the muscles although we performed MRI 3 to 5 days after the onset. This result did not match the results of the aforementioned studies.
Acute, subacute, and chronic stages were defined by shortening the generally used period classification to evaluate the usefulness of early diagnosis. According to our results, early diagnosis before chronic denervation was possible in 74%(26/35) cases. This fact, despite the lack of adequate sample size, calls for the need to further study the usefulness of MRI.
EDX changes occur within the affected muscles after denervation, which can be demonstrated on EMG7). It has been shown experimentally that early detection of spontaneous activity of the affected muscle is possible. However, the EMG changes are considered to occur late, justifying the clinicians to delay the exam for at least 2 weeks from the injury4,6). In addition, EDX is generally known for its invasiveness4,6,11). In our study, all subjects showed abnormal EDX findings, and 27 (77%) patients had muscle denervation. The detection rate of denervation was similar to the early diagnosis rate of MRI.
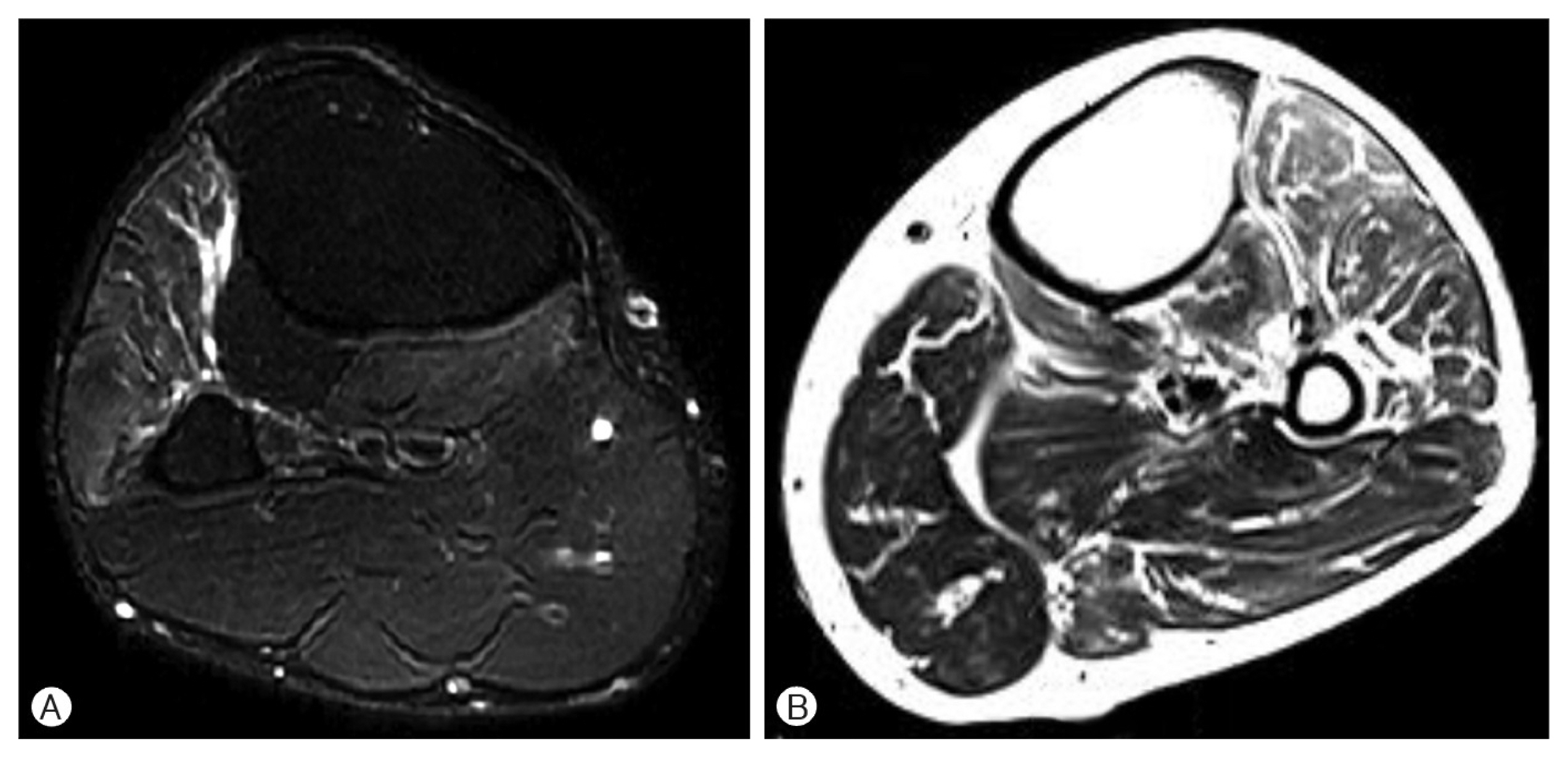
We would like to briefly present 2 cases demonstrating the usefulness of MRI in the diagnosis of CPNe. A 52-year-old male patient presented to our clinic with a chief complaint of right-sided progressive dropped foot 2 weeks prior to consultation. On admission, a positive Tinel sign was found on the fibular neck, and neurologic examination revealed ankle dorsiflexion Grade 3/5, big toe dorsiflexion Grade 3/5, ankle eversion Grade 4/5, and ankle inversion Grade 5/5. MRI showed muscle swelling of the anterolateral compartment without atrophy (Fig. 2A). Given these results, the diagnosis of right-sided CPNe was made, and the patient was advised to wait for spontaneous recovery. After 1 month, EMG revealed muscle denervation compatible with CPNe. In this case, we were able to make an early diagnosis based on both MRI finding and clinical manifestation prior to EDX, due to the required waiting time for detection.
In another case, a 55-year-old male patient visited our clinic with sudden onset of left-sided dropped foot 3 months prior to consultation. On admission, neurological examination revealed ankle dorsiflexion Grade 1/5, big toe dorsiflexion Grade 2/5, ankle eversion Grade 2/5, and ankle inversion Grade 5/5. EMG showed muscle denervation related to the CPN, and MRI revealed fatty infiltration with atrophy of the antero-lateral compartment of the lower extremity (Fig. 2B). We diagnosed the patient with left-sided CPNe and performed external neurolysis and decompression via the fibular tunnel approach. At the 1-month follow-up after surgery, there was an improvement in muscle strength. In this case, we could observe the EMG findings of denervation atrophy were well portrayed in the MRI as fatty infiltration in the muscle and the shrinkage of muscle volume.
Both EMG and MRI can diagnose muscle denervation and document the time course of muscle atrophy4,6,11). However, considering the invasiveness and time-consuming aspect of EDX, and as MRI can portray the electrophysiological and histological changes after denervation, MRI can be an effective tool for localizing and defining the extent of CPNe4,6,9,12).
This study has some limitations. First, as a retrospective study from a single institution, there was potential for several biases. Second, we enrolled a small number of patients; thus, the results of our study cannot be generalized.