INTRODUCTION
Hypertrophic pachymeningitis (HP), first described by Charcot and Joffroy in 18694), is characterized by rare inflammatory fibrosis and diffuse thickening of the dura mater 9). This disease can appear in the brain and spine with the dura mater. Progressively worsening chronic headache is the most common clinical symptom, along with various neurological symptoms such as multiple cranial nerve palsy and ataxia10,11). HP can be caused by autoimmune diseases, as well as by diseases that can cause dural reactions, such as infections, tumors, and intracranial hypotension syndrome, however, the idiopathic cause is reported in most cases1).
Although there are characteristic imaging findings, HP is difficult to diagnose at an early stage because it can be mistaken for other diseases, such as tumors or hematomas16). The gold standard for HP diagnosis is confirmation through biopsy. If appropriate treatment is not performed before an invasive procedure, the patient's prognosis may deteriorate.
This article describes a case of HP after burr hole trephination for chronic subdural hemorrhage (CSDH). To our knowledge, this is a rare case that has not been reported thus far.
CASE REPORT
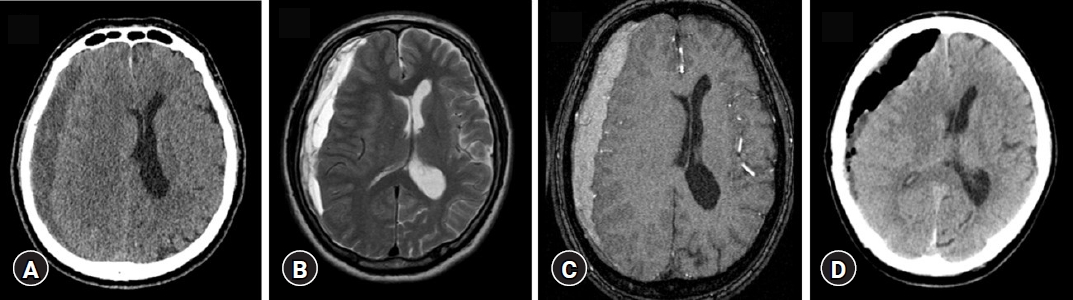
A 64-year-old male patient was admitted to the emergency room with a headache (visual analog scale [VAS] score 4) that started approximately 2 weeks prior. He had no underlying disease, and the history of trauma was unclear. After the diagnosis of CSDH via computed tomography (CT) (Fig. 1A) and magnetic resonance imaging (MRI) (Fig. 1B, C), burr hole trephination was performed (Fig. 1D).
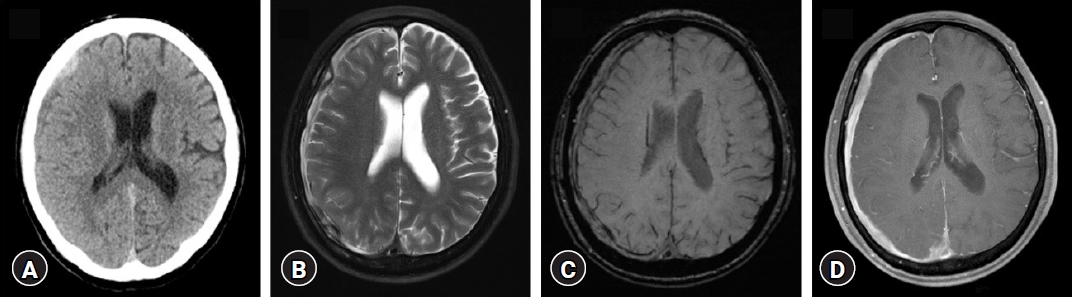
Six months after the operation, CT (Fig. 2A) and MRI (Fig. 2B-D) were performed for severe headache (VAS score 8) that recurred, and a second craniotomy was performed for recurrent subdural hemorrhage (SDH). A solid subdural granuloma was suspected and pathological examination revealed acute and chronic suppurative inflammation. Tissue biopsy and culture results did not reveal any abnormalities. After surgery, short-term oral prednisone (5 mg daily) was administered for 2 weeks, the patient's symptoms improved, and he was discharged.
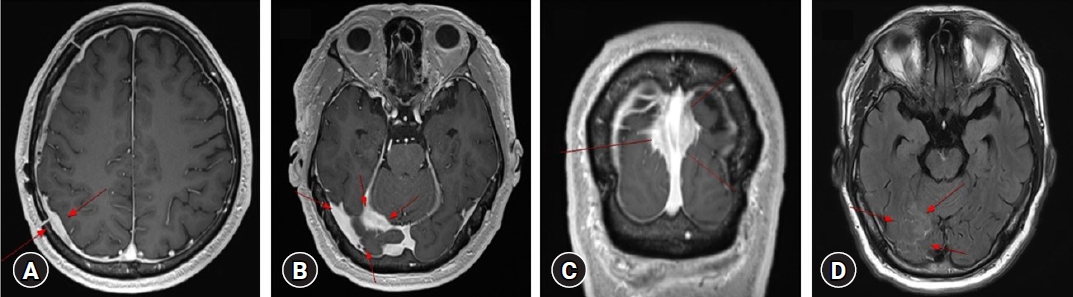
However, after 3 months, he visited the hospital with a severe headache (VAS score 8). MRI showed no significant difference in the area of the previous operation; however, focal venous congestion and localized venous ischemic or inflammatory changes were observed in the tentorium. Thickening of the right frontoparietal convexity (Fig. 3A) and right tentorium (Fig. 3B, D) was observed, and similar dural thickening was observed along the superior sagittal sinus (Fig. 3C).
A craniotomy was performed for biopsy, and the dura mater was remarkably thickened. The thickened dura mater was removed, and a biopsy was performed (Fig. 4A, B). Pathological examination revealed lymphoplasmacytic infiltrates with a fibrotic background. Immunohistochemistry revealed mixed T and B lymphocytes and plasma cells (Fig. 4C). IgG4+ plasma cells were also observed; however, the ratio of IgG4/IgG plasma cells did not exceed 40%.
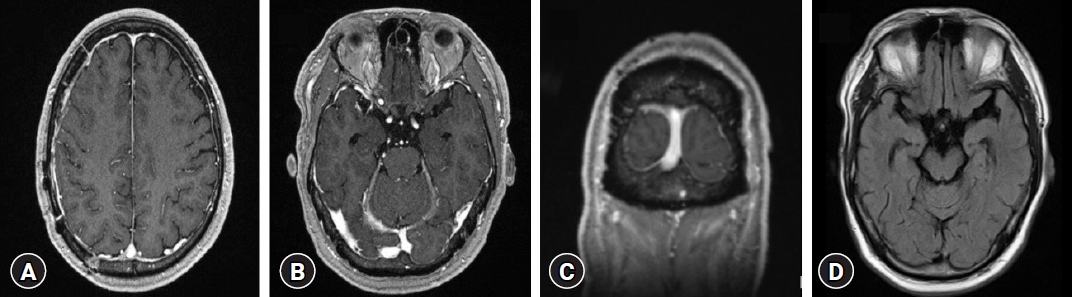
Additionally, cerebrospinal fluid (CSF) test, immunochemistry, blood laboratory, chest CT, and abdominal CT were performed to rule out systematic autoimmunity and infection accompanying tuberculosis, and no specific findings were found. Microbiological and molecular analysis on CSF did not show any evidence of infectious disease; the analysis included an extensive panel of bacterial, viral (Epstein-Barr virus, cytomegalovirus, varicella zoster, herpes simplex, human herpesvirus, rubella, adenovirus, Enterovirus), mycobacterium tuberculosis complex, fungal (Cryptococcus) infections. Intracranial pressure was 130 mmH2O which was within the normal range, and glucose (69 mg/dL), protein (28.5 mg/dL) lactate dehydrogenase (<25 mg/dL), pH 7.5, cell count (4 cell/μL), neutrophil (0%) were also within the normal range. Rheumatoid factor, antinuclear antibodies, anti-double-stranded DNA, anti-neutrophil cytoplasmic antibodies (ANCA; perinuclear-ANCA and cytoplasmic-ANCA), and anti-SS A and B were negative, leading to a conclusive diagnosis of HP. The patient was treated with intravenous dexamethasone (15 mg daily), followed by maintenance treatment with oral prednisone (40 mg daily), and an immunosuppressive agent (azathioprine, 100 mg). The dosages of prednisone and azathioprine were reduced after 3 months, and a follow-up MRI was performed after 6 months. The patient's symptoms improved after treatment with steroids and immunosuppressants. On the MRI performed six months after treatment, the abnormal signal change and enhancement along the right occipital and both parietal lobes had disappeared, and the patient no longer complained of headaches (Fig. 5). One year later, follow-up MRI showed no specific findings, and the patient remained asymptomatic.
DISCUSSION
HP is a rare inflammatory fibrosis with diffuse thickening of the cerebral and/or spinal dura mater that may cause a compressive effect or vascular compromise. It can present focally in the dura of the falx, tentorium, and cavernous sinus or in a diffuse pattern characterized by total intracranial or spinal dura mater thickening2). The causes of HP are diverse and include autoimmune disorders such as Wegener’s granulomatosis, rheumatoid arthritis, perinuclear-ANCA-positive diseases, and infectious diseases such as meningitis, tuberculosis, and fungal infections1,8). It can also occur in primary dural tumors, such as meningioma or dural lymphoma, as well as in diseases, such as IgG4-related disease and sarcoidosis13).
MRI is a useful tool for diagnosing HP. Gadolinium-enhanced T1-weighted MR images show characteristic dural enhancement and thickening3). However, these characteristics alone can often be mistaken for those of other diseases. Park et al. 9) reported a case in which idiopathic hypertrophic cranial pachymeningitis was misdiagnosed as an acute subtentorial hematoma, and Jung et al.6) reported a case in which granulomatosis with polyangiitis-associated HP was mistaken for spontaneous intracranial hypotension. Yao et al. 15) presented a large (71 × 34 × 27-mm) extra-axial mass at the right frontal convexity with severe edema mimicking meningioma. This lesion revealed a large number of infiltrated lymphocytes with fibrosis and microabscess formation on histopathological examination, and was eventually diagnosed as intracranial idiopathic HP. Because it is difficult to differentiate HP using only images, a dural biopsy is required for the etiological diagnosis of HP. The histopathological findings include fibrosis and thickening of the dura with chronic inflammatory cell infiltration (lymphocytes and plasma cells). Inflammatory infiltration activates fibroblasts and induces collagen deposition, leading to tissue hypertrophy and increased dural thickness14).
Our case was CSDH, which was thought to have recurred after surgery, but it was confirmed by hypertrophic dural thickness, not hemorrhage. This can be diagnosed as iatrogenic or idiopathic HP. We found no reports of HP that occurred after burr hole trephination surgery or CSDH, which makes this a rare case. One study reported the relationship between CSDH and dura mater fibrosis. Charleston and Cooper5) performed a pathological examination of a hematoma in a patient diagnosed with CSDH who underwent surgery. Pathology of the hematoma revealed fibrous thickening of the inner layer of the dura mater, with thickened small vessels surrounded by inflammatory infiltrate, which was defined as “internal hemorrhagic pachymeningiosis”. Although its pathogenesis is unknown, it has been reported that relaxation and dissociation occur in the fibers of the inner layer of the dura mater, resulting in chronic and fibrous thickening of the dura mater. However, these cases were resolved with burr hole surgery for CSDH and showed no other complications. In our case, it was in the form of a thickened dura, not a hematoma of “internal hemorrhagic pachymeningiosis,” and considering that it was eventually resolved through the use of immunosuppressive agents and steroids, HP seems reasonable.
The clinical manifestations of HP may vary depending on the lesion location; however, chronic headache is the most common symptom5). Involvement of the dura mater causes headache, which is usually global, chronic, and severe, and often does not improve with analgesics or nonsteroidal anti-inflammatory drugs13). Compression of the cortical vessels and inflammatory infiltration into the brain parenchyma can cause venous congestion and ischemia, which can make headaches worse1). In our case, chronic headache was the main symptom, and the patient experienced severe pain because it was not controlled by medication. The two factors mentioned are thought to have caused severe headaches.
There are no randomized clinical trials for the treatment of HP, and clear standard guidelines for doses are controversial; however, there is consensus on corticosteroid therapy as a first-line treatment. In previous literature reports, Prednisolone (0.6-1 mg/kg/day) and methylprednisolone (1 g/day for three days) are generally administered initially, followed by follow-up of the patient's symptoms and imaging tests, tapering of steroids, and further treatment7,11,16). However, in cases of refractory disease or relapse after steroid use, immunosuppressive agents such as azathioprine, cyclophosphamide, methotrexate, and mycophenolate mofetil are effective12,14). In addition, high-dose steroids were more effective than low-dose steroids in relieving the symptoms of chronic headaches. After diagnosing HP, we used a high-dose steroid at a lower dose than the dose recorded in reports in various literature. It was judged that HP had progressed with the use of oral prednisone in the past, and the symptoms could be alleviated by the anti-inflammation effect of steroids, but the disease could be aggravated. Therefore, the use of immunosuppressive drugs was judged to be effective for the patient, so steroids were not started at full dose. We confirmed that the patient's symptoms were alleviated and the lesions disappeared from the images.
CONCLUSION
Herein, we report a rare case initially mistaken for CSDH and histologically confirmed as Idiopathic HP after surgery. It is difficult to differentiate between SDH and HP based on radiographic findings alone. If a patient complains of persistent headaches after surgery for chronic SDH, a dural biopsy can be a treatment option for differentiation. If the final diagnosis is made histologically, prompt use of steroids improves the patient's prognosis.